Breast Lesions
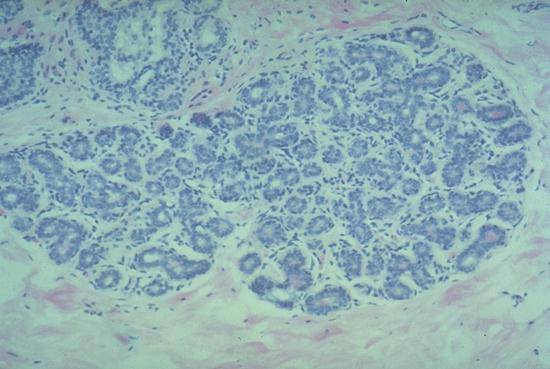
Each duct and/or "acinus" is lined by two epithelial cell layers, an inner cuboidal layer, and an outer often less visible myoepithelial layer.
In this low power view, one can see a distorted lobule surrounded by fibrous tissue. The ducts in the center are severely compressed and squeezed into flat shapes that, to the unwary, resemble infiltrating carcinoma. Nearer the periphery the ducts "open up" and have a more normal appearance. Key features that distinguish it from carcinoma are the fact that it is a process that affects single lobules and that it selectively distorts the central part of the lobule.
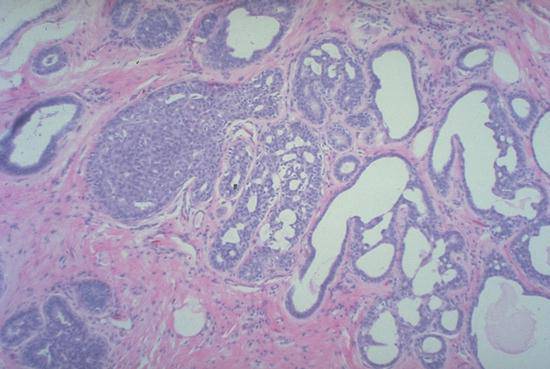
Epitheliosis is characterized by proliferation of benign epithelial cells filling ducts, a process which tends to be multicentric.

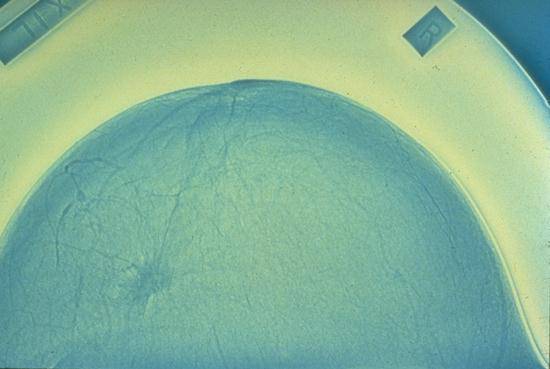
Benign cysts filled by serous fluid often have this blue color when viewed from the outside.

Cysts of various size are interspersed by dense fibrous tissue. This patient, who was in a high risk category for breast carcinoma, elected to have bilateral mastectomies with prosthetic implants. This degree of "fibrocystic change" becomes impossible to follow on mammograms due to complex shadows from the dense fibrous tissue.

The pale grey cut surfaces show a bulging glistening appearance due to the predominant loose fibrous stroma rich in mucopolysaccharides. Note well defined outline.
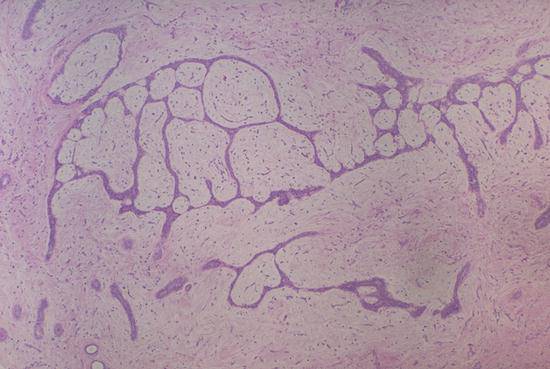
Fibroadenomas are a co-proliferation of both glands and stroma (connective tissue). The stroma usually has a watery blue "myxoid" appearance. Stromal proliferation frequently distorts the glands into complex, anastomosing, ribbon-like profiles as shown here.
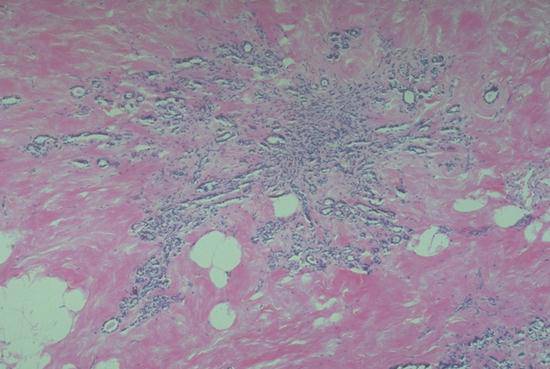
A "superior" view of a large fatty (therefore translucent) breast with the classical "stellate" or "crab-shaped" dense appearance of an invasive carcinoma.

The central irregular chalky white, retracted area is the invasive carcinoma surrounded by the normal yellow fatty breast tissue. (The black on the surface of the specimen is India ink used to delineate surgical margins.)
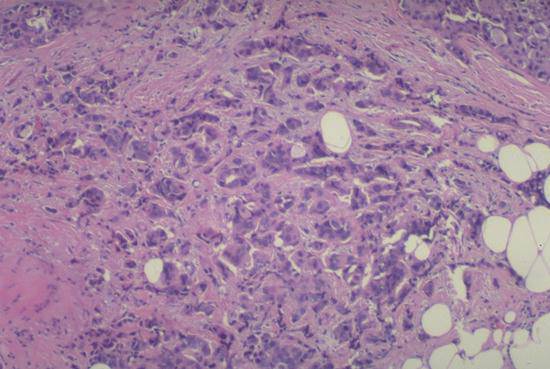
This is the most common pattern. Small nests, cords and occasional gland-forming groups of cells infiltrate the fibrous stroma in an irregular manner. Some tumor cells extend into fat. Virtually all the cells are cancer cells.
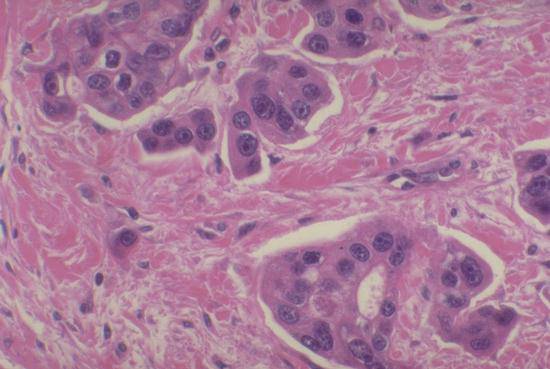
At higher power, one can appreciate the two features that distinguish ductal from lobular carcinoma: high nuclear grade (anaplastic cytology) and formation of duct-like structures.
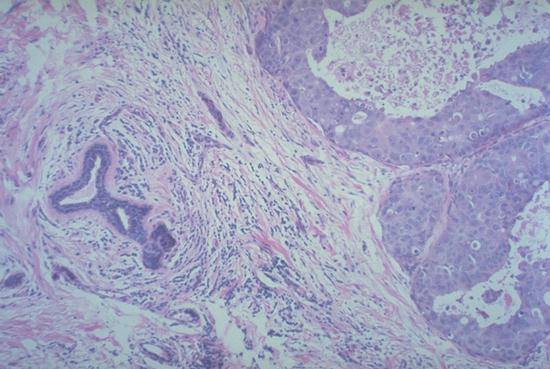
An intraductal carcinoma which usually shows many ducts distended by large malignant cells and central necrosis. Note the two large ducts with cancer on right in contrast to smaller benign ducts in the center.
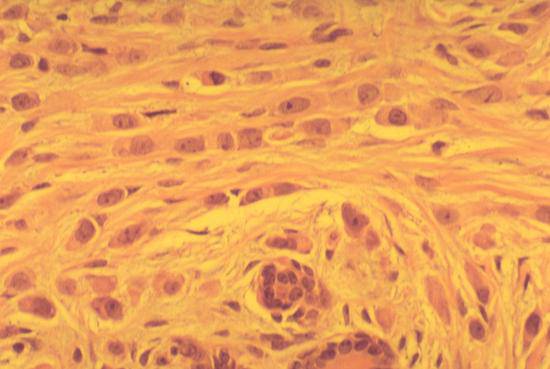
Contrast the relatively small size, uniformity, and minimal nuclear atypia of these infiltrating cancer cells with those of infiltrating ductal carcinoma (BR18). Note the "indian file" pattern of infiltration and the absence of gland formation.
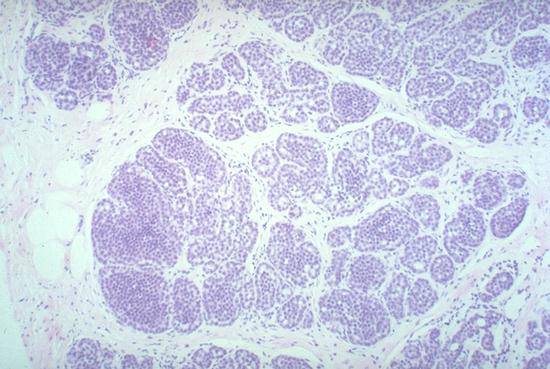
A distinctive pattern with a "bags of marbles" appearance. The neoplastic cells here are small, uniform, bland and distend the acinar units within a lobule.
(Compare to normal lobule in #1)
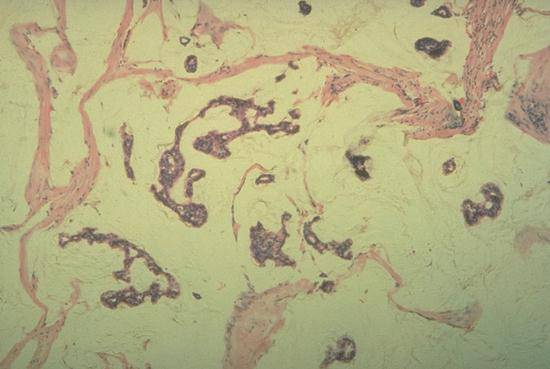
The tumor cells secrete abundant mucin which dissects the stroma. The cells appear to "float" in this pale background of mucoid material. These tumors are often bulky due to their mucin content.

The normal lobule shows two adjacent lymphatic spaces containing clusters of large malignant cells. This is typically seen in aggressive "high grade" or poorly differentiated carcinoma, which spreads rapidly via the lymphatics (e.g. as seen in "inflammatory carcinoma" of breast).

Drainage is chiefly to the axillary lymph nodes.

Right Breast Carcinoma, Autopsy Case A71-205 - Clinical. This patient, a 44 year old white female with a 1 1/2 year history of right breast mass and pain, refused hospitalization for a probable carcinoma of the right breast when seen by her doctor six months prior to admission. Four weeks prior to admission, the patient developed nausea, vomiting, coughing, shortness of breath, fatigue and increasing weakness. Physical examination on admission revealed a very weak female with a right breast mass with "peau d'orange" skin retraction, muscle retraction, and nontender axillary lymphadenopathy. These features are recognizable on this slide. Chest x-ray revealed the diffuse lymphangitic spread of carcinoma on the lungs bilaterally with a questionable invasion of rib and calcification of the right axillary lymph node. White blood cell count was 13,4000 with a marked shift to the left. She was placed on a 5 drug protocol for metastatic carcinoma of the breast consisting of prednisone, cytoxan, Vincristine, Methotrexate, and 5-fluorouracil. On her fourth hospital day the patient had a biopsy of a nodule of skin overlying the right breast. Then on the fifth hospital day a bone marrow aspirate and biopsy were done; these revealed tumor cells.