Gastrointestinal: Colorectal Neoplasms

Tubular adenoma of the colon. This lesion was removed with snare-electrocautery during colonoscopy. Note the stalk of normal tan mucosa and the multilobulated head of the polyp. The stalk is formed when the polyp grows to a size that allows it to be pulled on by peristaltic forces.

Histologic section of tubular adenoma. Note the stalk composed of normal mucosa ending abruptly at the junction with the adenoma. Compare the architecture of the crypts in the normal mucosa of the stalk with the distorted architecture in the adenoma. There is no evidence of invasive carcinoma in this adenoma.
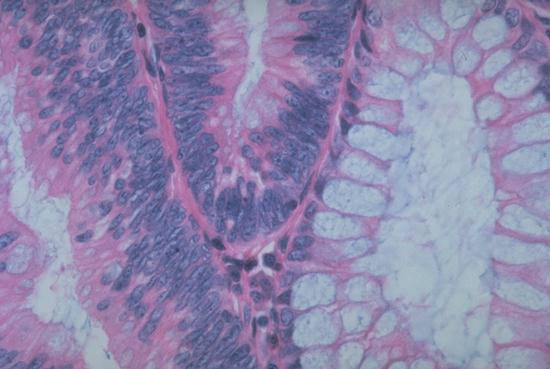
This photomicrograph of a tubular adenoma shows a normal crypt to the right. Note the prominent goblet cells and the single row of basally oriented small nuclei. The other two crypts in this field show decreased mucus secretion and marked crowding and stratification of the slightly enlarged nuclei. This contrast between the appearance of the normal and the neoplastic epithelium is characteristic of glandular lesions throughout the GI tract.

Adenocarcinoma of colon. This en face view of an opened colon shows a typical circular carcinoma with elevated, heaped-up edges and central ulceration.

Adenocarcinoma of colon. This cross section through a colonic carcinoma shows a fungating, polypoid lesion with a central ulceration. A short strip of normal colon is present on the left edge of the specimen; the muscularis propria is gray and translucent compared to the white fibrous tissue above and below it.. Note that the white tumor extends through the colonic wall into the pericolonic adipose tissue. Patients whose cancer extends through the bowel wall but has not metastasized have an approximately 75% probability of cure by surgical treatment alone. If they have metastatic carcinoma in the lymph nodes, then the probability of cure falls to around 30%.
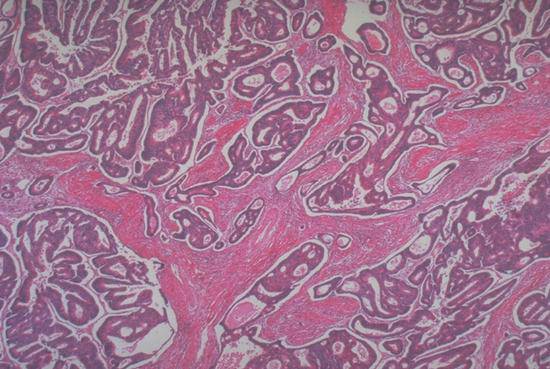
This low power photomicrograph of a colon carcinoma shows architectural abnormalities that are even more severe than those of an adenoma. Note especially the eosinophilic bands of desmoplastic connective tissue between the nests of infiltrating carcinoma. Desmoplasia (stimulation of benign fibroblasts to produce large amounts of extracellular matrix) is a feature of invasive tumors, not in situ disease.