Gastrointestinal: Gall Bladder/Bile Ducts/Pancreas
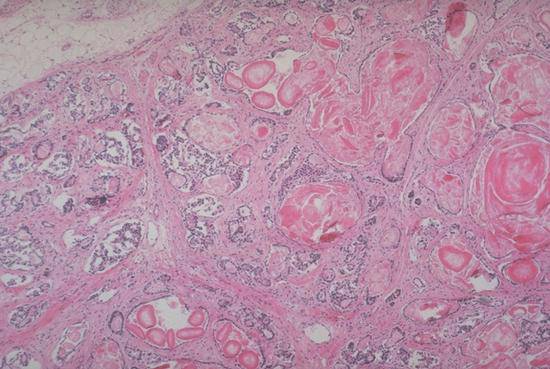
Fibrocystic disease of the pancreas (cystic fibrosis). The genetic defect in fibrocystic disease results in the production of abnormally viscid secretions from exocrine glands. In this photomicrograph of the pancreas, these secretions can be seen as rounded, eosinophilic masses distending and obstructing pancreatic ducts. This has resulted in destruction of much of the exocrine parenchyma with subsequent fibrosis of the interstitium.
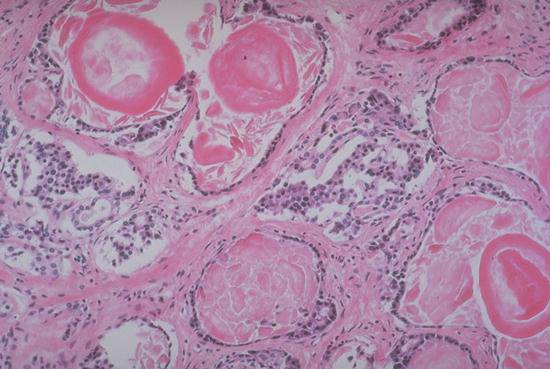
In this higher power view of the same pancreas, the abnormal secretions can be readily seen within the dilated ducts. There is no normal exocrine parenchyma remaining, however normal islet tissue is present at the left center and near right center of the field.
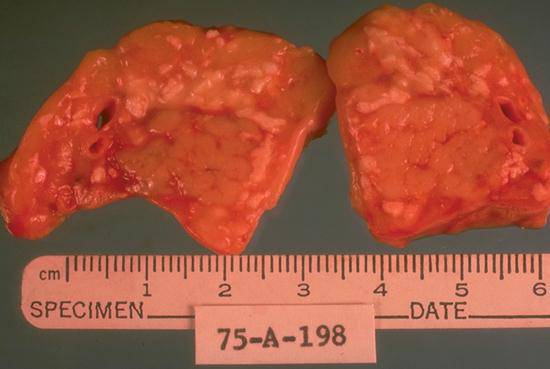
This cross sections of a pancreas from an autopsy shows the chalky whitish-yellow appearance of fat necrosis that indicates the pancreas has acute pancreatitis. Pancreatic lipase releases fatty acids from the triglyceride molecule which then form calcium soaps that produce this whitish-yellow appearance.
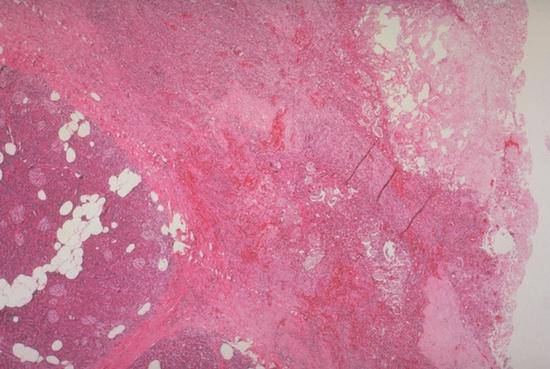
This slide shows the microscopic appearance of the pancreas illustrated in the previous slide. Normal pancreatic parenchyma can be seen at the lower left portion of the field and necrotic adipose tissue in the upper right portion. The two are separated by an inflammatory reaction.
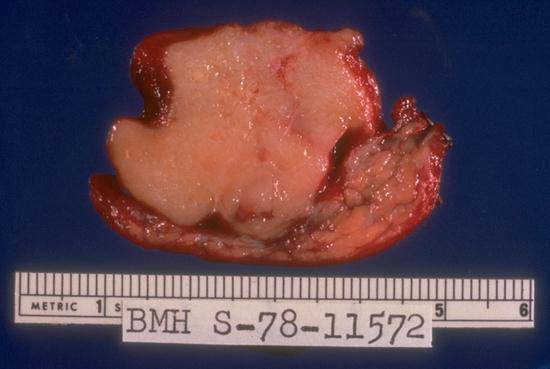
This specimens was removed from a 20 year-old female with chronic diarrhea and a mass detected in the pancreas. Note the smooth, homogeneous appearance and sharply circumscribed margins of the neoplasm. This is the characteristic gross appearance of an islet cell or endocrine neoplasm.
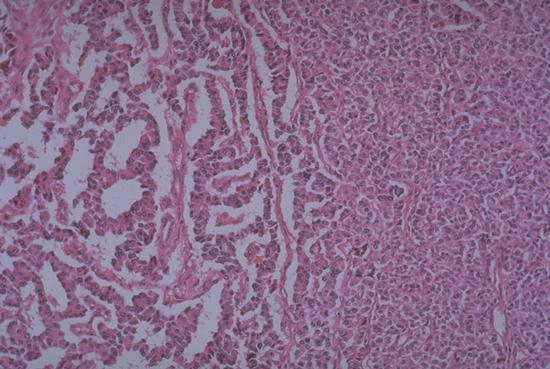
This photomicrograph of the islet cell tumor shows the characteristic ribbon-like pattern of islet cell tumors to the left while to the right the neoplasm grows in more solid sheets.
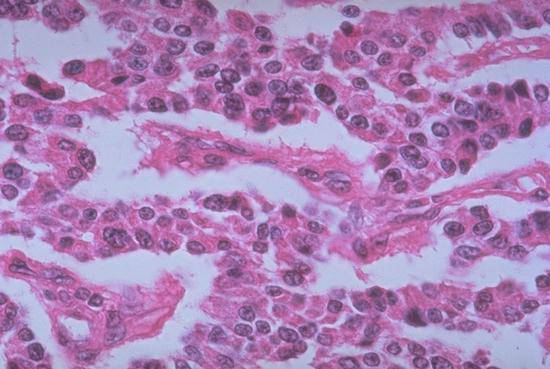
At higher power, the endocrine cells composing the neoplasm can be seen to have relatively round, uniform nuclei and granular eosinophilic cytoplasm.
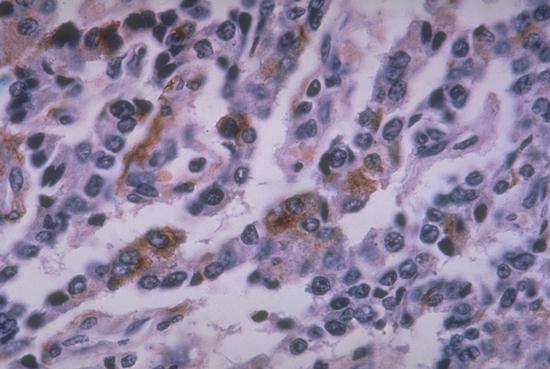
This illustrates the results of application of a monoclonal antibody directed against somatostatin to the neoplasm. The brown reaction product indicates binding of somatostatin antibody to somatostatin within the cytoplasm of the neoplastic cells. The production and release of somatostatin by this tumor results in the patient's diarrhea.

This slide shows an opened gallbladder specimen containing numerous gallstones (cholelithiasis), a major cause of morbidity in the USA.

This gross specimen shows a tumor mass of the head of the pancreas, seen in the center of the photo, surrounded by duodenum, resected together as part of a Whipple procedure for pancreatic adenocarcinoma.
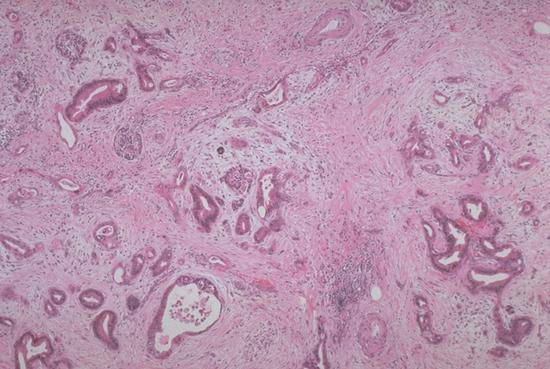
This photomicrograph shows the microscopic appearance of pancreatic ductal adenocarcinoma, an almost uniformly fatal cancer. Over 90% of malignant pancreatic tumors are ductal in origin, as seen here with invasive disordered malignant glands.