Respiratory: Lung Cancers
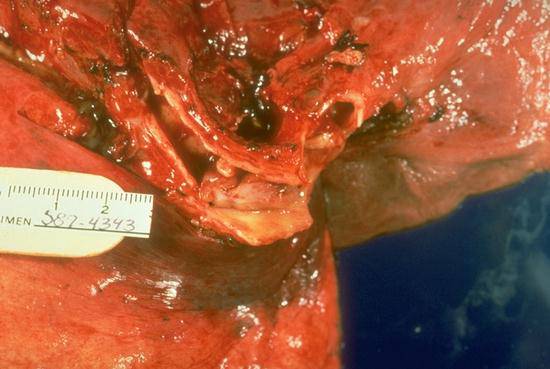
There is a pale, gray-white smooth polypoid lesion within the opened bronchus. It is near the end of the ruler and measures approximately 2cm in diameter. This illustrates the typical central location of carcinoid tumors as well as their most common growth pattern; i.e. a polypoid endobronchial mass. These tumors usually come to attention because of symptoms related to endobronchial obstruction. These tumors are highly vascular and bleed extensively following an endobrochial biopsy.
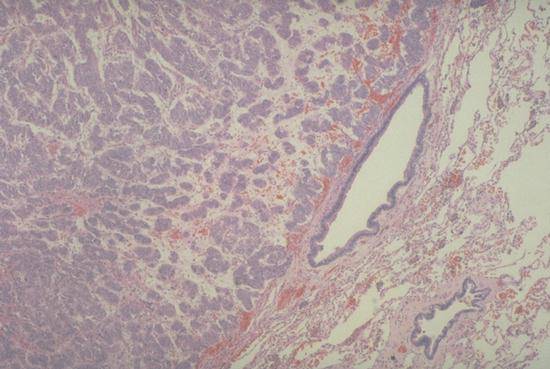
This low power photomicrograph illustrates the characteristic "pushing" border of the tumor. It also illustrates how the blue tumor cells are organized into small fairly uniform packets or bundles. A rich network of capillaries surrounds the cell bundles. The recapitulates the normal organization of neural endocrines cells wherein the cells produce neurotransmitters and secrete them into adjacent capillaries. Carcinoid tumors usually do not metastasize but it is best to consider them low grade carcinomas.
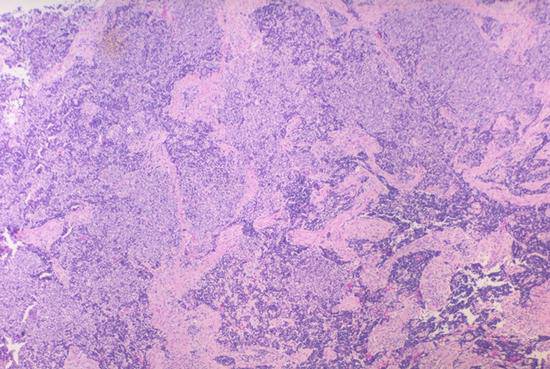
In contrast to the well-organized groups of tumor cells in carcinoid tumors, the cells in small cell carcinoma are usually arranged as featureless, disorganized sheets. The totally disorganized growth in this low power photomicrograph is typical of small cell carcinoma but non-small cell carcinomas may also occasionally show this growth pattern. Crush artifact is common; partially crushed cells stain darker blue.
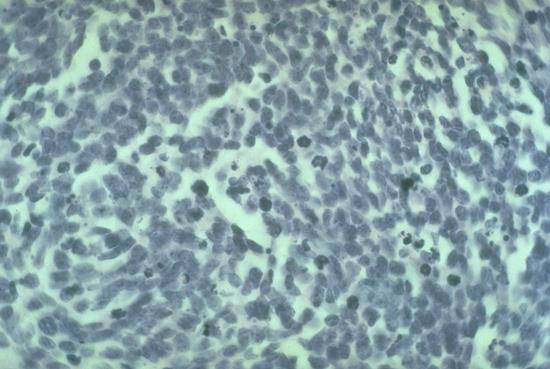
This high power photomicrograph illustrates the characteristic cytologic appearance of small cell carcinoma. The cells have virtually no discernable cytoplasm and the nuclei are relatively uniform in size. Dense blue-staining material is scattered through this microscopic field. This represents individual cell necrosis in some cases and mitotic figures in others. The nuclei are about twice the diameter of red blood cells.
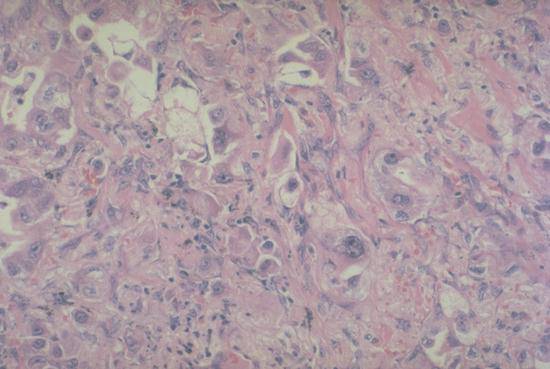
Adenocarcinomas exhibit a variety of growth patterns. In this medium power photomicrograph, the cells are quite variable in shape and size and are arranged in disorganized nests and sheets. Occasional cells have a vacuolated cytoplasm, which corresponds to intracytoplasmic clear mucin. Note how large these nuclei are compared to red blood cells.
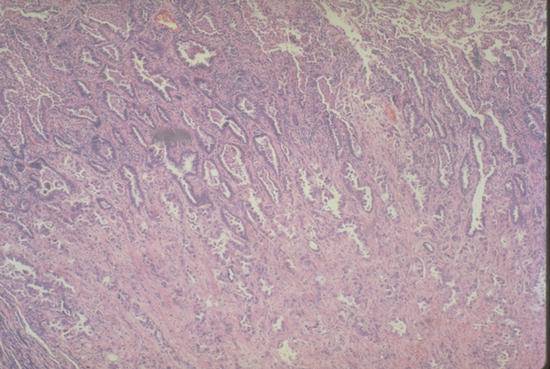
Often, adenocarcinomas will spread over the preformed alveolar network to a greater or lesser extent around the periphery of the main tumor. This is illustrated in the low power photomicrograph where a relatively solid central area of carcinoma merges into a broad zone where the tumor cells line distorted alveolar spaces. A small amount of normal alveolar lung tissue is present in one corner. The amount of spread over preformed alveolar septa has little bearing on the prognosis.
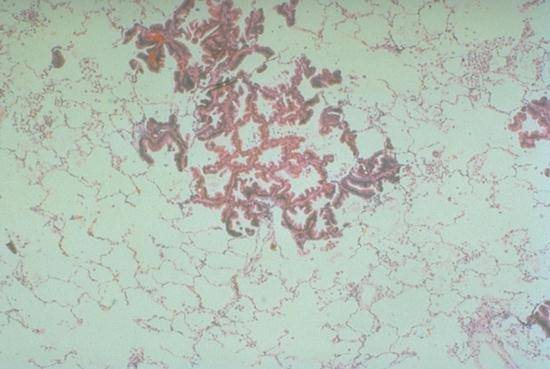
Unusual variants of adenocarcinoma that grow exclusively over alveolar septa, such as this case, are called bronchioloalveolar carcinoma. These tumors, which have not invaded the underlying interstitium, generally do not metastasize to lymph nodes but rather grow by spreading over the surfaces that line the alveoli throughout the lungs. Some of these tumors produce copius amounts of mucous and patients may suffer bronchorrhea.
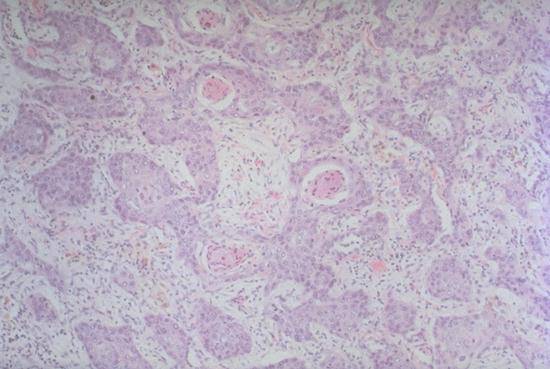
The hallmark of squamous cell carcinoma is evidence of keratinization. This may be either the formation of "keratin pearls" as in the centers of these tumor nests, or intercellular bridges as in the next picture. Squamous cell carcinomas arise in the central conducting airways more commonly than do adenocarcinomas.

This oil immersion high power photomicrograph illustrates an extensive network of intracellular bridges that links adjacent cells. Extensive intracellular bridges are a diagnostic feature of squamous cell carcinoma.
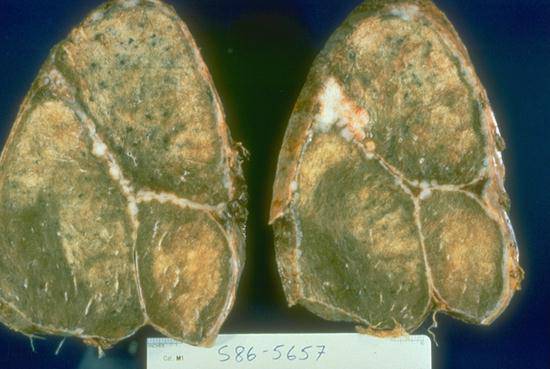
Mesothelioma, which arises on the pleural surfaces, spreads over the pleural surfaces in a characteristic pattern. The white tumor nodules visible on these slices of the right lung, are arranged around the periphery of the lung as well as in the major and minor fissures. Mesotheliomas tend not to invade the lung parenchyma until they are very advanced.