Vasculitis
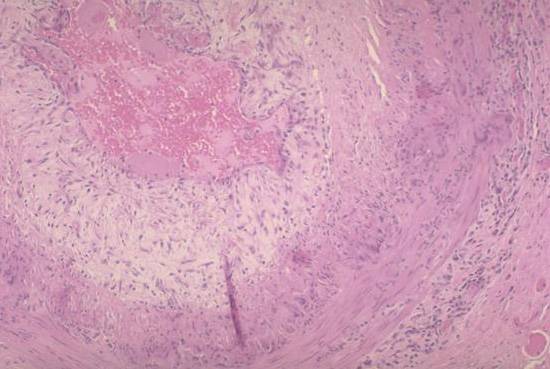
This medium power photomicrograph shows a florid example of giant cell arteritis. The most characteristic feature is the ring of granulomanous inflammation that seems centered around the elastic lamellae within and bounding the media. Note the well formed multinucleated giant cells at 3 o'clock. Notice also the large pale zone of intimal thickening and fibrosis as well as the central acute thrombus. A moderate nonspecific inflammatory infiltrate is present in the adventitia.
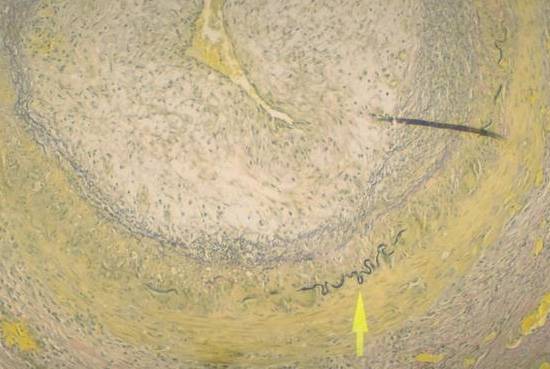
In this stain, elastic tissue appears black while various types of collagen stain yellow. Notice the remnants of the internal elastic lamina at the arrow. If you look carefully, you can see multi-nucleated giant cells and macrophages which appear to be attacking the elastic tissue and ingesting it. As in the previous photograph, there is extensive intimal proliferation and fibrosis.
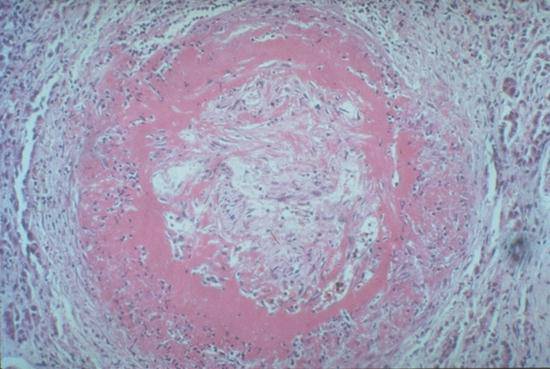
Note the prominent eosinophilic "fibrinoid" necrosis involving the intima and media of this muscular artery. In contrast to giant cell arteritis, there is no granulomatosis inflammation. Notice also how the lumen has been occluded by granulation tissue.
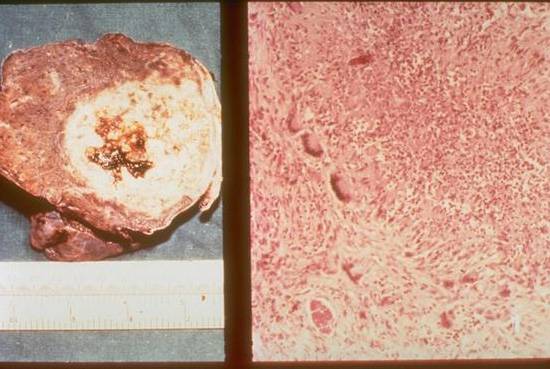
The left panel of this composite photograph shows the irregular macronodular appearance that Wegener's granulomatosis may assume in the lung. The white nodular mass is fairly sharply demarcated from the surrounding brown parenchyma. There is central hemorrhage and necrosis within the mass. In the right panel, one can appreciate the characteristic irregular zone of necrosis with many small condensed cells (probably neutrophils) near the center. These are surrounded by multinucleated giant cells and spindle shaped macrophages to form a characteristic palisading granuloma. Dense reactive fibrous tissue surrounds the layer of macrophages and giant cells.
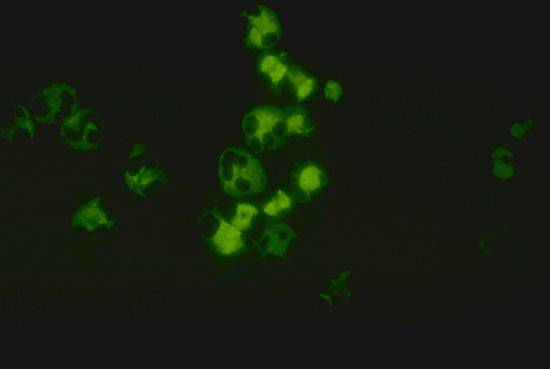
In this test, normal neutrophils are placed on a dish, then incubated with a sample of the patient's serum. Unbound antibodies from the patient's serum are then washed away and a fluorescent antibody against immunoglobulins is placed over the neutrophils in order to detect antibodies from the patient's serum that are bound to the neutrophils. In this high power photomicrograph, positive green fluorescence can be seen throughout the cytoplasm of the labeled neutrophils. The non-staining polylobated nuclei stand out against the cytoplasmic fluorescence.
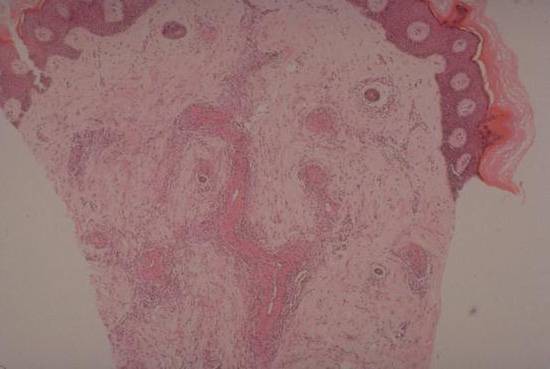
This low power photomicrograph of a deep skin biopsy shows how this vasculitis preferentially involves the small vessels of the mid and deep dermis. These vessels display extensive bright pink "fibrinoid" necrosis. They are surrounded by cuffs of inflammatory cells. Often, patients with vasculitis may hemorrhage from the involved vessels, leading to clinically evident purpura.
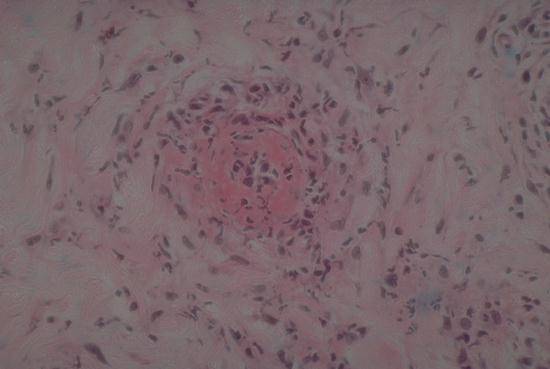
This higher power photomicrograph shows a cross section of a small vessel with extensive fibrinoid necrosis and surrounding inflammatory cells. This pattern of reaction happens to have been caused by a hypersensitive reaction to a drug in this patient, but the histopathologic findings are identical to small vessel vasculitis due to other causes.